Introduction
Clearing active acne feels like a victory — until you look in the mirror and see what it left behind. Scars, pits, and discolouration can linger long after the breakouts stop, and for many people, they're harder to accept than the acne itself.
The numbers reflect this reality. A 2023 meta-analysis of 37 studies and 24,649 patients found that scarring occurs in roughly 67% of moderate acne cases and 82% of severe acne cases — making post-acne scarring one of the most common skin concerns dermatologists manage.
One important point: active acne must be controlled before scar treatment begins. Ongoing breakouts create new scars and reduce the effectiveness of any resurfacing or collagen-rebuilding procedure.
This guide covers how scars form, what separates one scar type from another, which at-home options actually help, and which clinical treatments deliver real results. It also addresses treatment considerations specific to Indian skin tones.
Key Takeaways
- Acne scars form when deep breakouts damage the dermis — the scar type (ice pick, boxcar, rolling, or raised) determines which treatment works
- OTC retinoids, AHAs, and salicylic acid address mild scarring — moderate-to-severe scars require clinical intervention
- Clinical options range from chemical peels and microneedling to subcision, fillers, and punch excision
- Darker Indian skin tones (Fitzpatrick IV–VI) need careful treatment selection to prevent post-inflammatory hyperpigmentation
- A personalised, dermatologist-supervised treatment plan consistently outperforms self-treatment
Understanding Acne Scar Types and How They Form
The Biological Mechanism
When a breakout penetrates deep into the dermis, it damages surrounding tissue. The skin's repair process kicks in — but it doesn't always get the balance right.
- Too little collagen during healing → depressed (atrophic) scars
- Too much collagen during healing → raised (hypertrophic or keloid) scars
Nodular and cystic acne are the most likely culprits, since they inflame tissue at the deepest levels. Picking, popping, or squeezing spots significantly worsens outcomes by pushing bacteria deeper and disrupting the natural healing process.
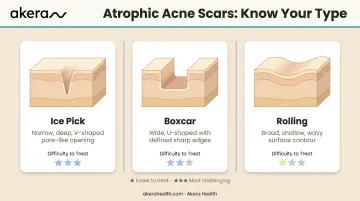
Atrophic (Depressed) Scars
These are the most common type on the face, and they come in three distinct forms:
| Scar Type | Appearance | Treatability |
|---|---|---|
| Ice pick | Narrow, deep, V-shaped tract | Hardest to treat — requires targeted techniques |
| Boxcar | Wide, U-shaped with sharp edges | Responds well to resurfacing procedures |
| Rolling | Broad, shallow with a wavy surface; caused by fibrous bands beneath the skin | Responds well to subcision + resurfacing |
Hypertrophic and Keloid Scars
Raised scars result from excess collagen production during healing. They're more common on the chest, back, and jawline than on the face.
- Hypertrophic scars stay within the original wound boundary
- Keloid scars grow beyond it — a more severe variant that requires a completely different treatment approach
Getting this distinction right before starting treatment matters — applying resurfacing techniques to a keloid can actively worsen it.
Post-Inflammatory Hyperpigmentation vs. True Scars
The flat red, brown, or purple marks left after acne clears are post-inflammatory hyperpigmentation (PIH) — not true scars. They involve no structural change to skin texture, which makes all the difference for how they're treated.
PIH can persist for 6–12 months in darker skin tones, and deeper dermal pigmentation can last even longer. But unlike true atrophic or raised scars, PIH will fade on its own without structural intervention. True scars — involving actual pitting or raised tissue — are permanent without active treatment.
At-Home Treatments for Acne Scars
At-home options work gradually and are most effective for mild surface-level scarring or PIH. For moderate-to-severe structural scarring, they serve as maintenance between clinical sessions — not a standalone fix.
Key Ingredients That Actually Help
Retinoids are the most evidence-backed topical option. A 2021 clinical review confirmed their effectiveness for acne-associated PIH in skin of colour. They speed up cell turnover and reduce discolouration — but they increase sun sensitivity, so daily SPF is essential when using them.
Other useful actives:
- Alpha hydroxy acids (AHAs) — glycolic and lactic acid exfoliate dead skin cells and gradually reduce surface discolouration
- Salicylic acid — penetrates pores, reduces redness and surface irregularity, works across scar types
One important caveat: high-strength acids (glycolic at 35%+, TCA) belong in a clinic. The at-home versions are milder and work on surface texture — they won't address deep structural scarring.
The Role of Daily Sunscreen
UV exposure darkens scars and makes PIH visibly worse. For Indian skin tones, where post-inflammatory pigmentation is more pronounced, daily broad-spectrum sunscreen is a baseline requirement, not an afterthought.
If you're managing acne alongside scarring, look for a sunscreen that won't clog pores. Akera Health's Bask Sunscreen (SPF 50+, ₹1,299) is formulated for oily and acne-prone skin — broad-spectrum protection without triggering new breakouts.
Setting Realistic Expectations
At-home care won't remove established ice pick scars, deep boxcar scars, or raised keloids. It can fade PIH, smooth mild surface texture, and maintain gains from clinical treatments. For anything beyond surface-level concerns, consult a dermatologist before starting any new regimen.
Clinical Treatments for Acne Scars
Clinical treatments are recommended for moderate-to-severe scarring. A dermatologist will assess scar type, depth, and skin tone before recommending a protocol — and often combines multiple methods for better outcomes than any single treatment alone.
Resurfacing Treatments
Chemical peels use a controlled chemical solution to remove the outer skin layer, revealing regenerated skin underneath. Peel strength is selected based on scar severity:
- Mild-to-medium peels can be repeated over several sessions
- Deep peels are typically a one-time procedure with longer recovery
- All peels carry a risk of pigmentation changes — particularly in darker skin tones
Akera Health's dermatologist-supervised chemical peels use plant-based solutions, starting from ₹3,000 per session — making them a practical option for mild-to-moderate surface scarring and PIH.
Laser resurfacing comes in two forms:
- Ablative (for example, fractional CO2) — removes the top skin layer; more aggressive with longer downtime
- Non-ablative — stimulates collagen without surface damage; lower risk, more sessions required
For darker skin tones, ablative lasers carry meaningful PIH risk. A 2014 study of fractional CO2 laser found that it was appropriate only for Fitzpatrick types II–IV, with PIH occurring in some participants. Non-ablative and fractional technologies are generally safer starting points for Indian skin.
Dermabrasion mechanically planes the skin surface using a rotating tool. Evidence is older and less standardised — a 2017 systematic review found microdermabrasion produced the least significant results among non-energy-based treatments.
Collagen-Stimulating Treatments
Microneedling uses a device with fine needles to create controlled micro-injuries, triggering collagen production. A primary study using 6 sessions estimated 51–60% improvement at 3 months in atrophic scars — though the study included only 10 patients, so individual results vary. Multiple sessions (commonly 4–6) spaced weeks apart are standard.
RF microneedling adds radiofrequency energy to standard microneedling, delivering heat deeper into the dermis for more significant collagen remodelling. An Indian study of 40 patients found a mean scar score reduction of 34.35% after 4 sessions, with a PIH rate of just 5% and erythema resolving within 24 hours — making it well-suited for Indian skin tones.
Akera Health offers Morpheus8 Pro RF Microneedling from ₹10,000 per session. Downtime is minimal — redness and swelling typically resolve within 48 hours — with scar texture improvements building over several weeks.
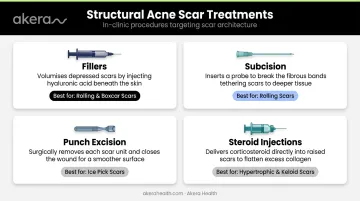
Structural and Targeted Treatments
For depressed, raised, or deeply tethered scars, dermatologists use targeted interventions:
- Fillers (hyaluronic acid) — injected beneath depressed scars to plump the surface; a 2024 clinical trial found improvement sustained through day 720. Best for rolling and distensible boxcar scars.
- Subcision — a needle or probe breaks fibrous bands tethering the scar to deeper tissue, allowing it to rise toward the surface. Usually followed by laser or microneedling to refine results.
- Punch excision — surgically removes individual deep ice pick scars; the sutured wound leaves a smaller, flatter mark that fades over time, then undergoes resurfacing once healed.
- Steroid injections (intralesional triamcinolone) — the standard approach for hypertrophic and keloid scars; injected directly into raised scar tissue across multiple sessions to flatten and soften it.
Choosing the Right Treatment for Your Skin and Scar Type
Matching Treatment to Scar Morphology
No single treatment works for every scar type. Here's a practical framework:
| Scar Type | First-Line Options |
|---|---|
| Ice pick | Punch excision, TCA CROSS |
| Boxcar | Resurfacing (peels, laser, dermabrasion), fillers |
| Rolling | Subcision followed by resurfacing or microneedling |
| Hypertrophic/keloid | Steroid injections, laser |
Combination approaches — using two or more treatments in a coordinated sequence — consistently deliver better outcomes than any single method. Which combinations work best depends heavily on your skin tone and how your skin responds to resurfacing.
The Indian Skin Tone Factor
Fitzpatrick types IV–VI (common among patients in Bengaluru) are more prone to PIH and adverse reactions from aggressive ablative lasers. An India-authored 2020 evidence review recommends morphology-based combinations using subcision or punch methods for deep/tethered scars and conservative resurfacing or collagen-induction methods for generalised atrophy in darker skin.
Key guidance for darker-skinned patients:
- Prefer non-ablative or fractional technologies over fully ablative resurfacing
- RF microneedling (like Morpheus8 Pro) carries lower PIH risk than ablative CO2 laser
- Chemical peels at appropriate strengths are well-tolerated — a split-face study found 6.7% PIH with glycolic acid versus 20% with TCA full-face peels
- Seek a dermatologist experienced with melanin-rich skin
What to Expect from a Dermatologist Consultation
At Akera Health, a dermatologist consultation covers:
- Detailed skin assessment and scar classification by type and depth
- Review of skin tone, genetics, and lifestyle factors
- Discussion of realistic timelines and outcome expectations
- A multi-step treatment protocol tailored to your specific scar profile
No single treatment eliminates scars completely. The realistic goal is significant improvement in scar depth and visibility, and that's very achievable when your protocol is built around your specific scar types, skin tone, and healing response. A structured, dermatologist-supervised plan makes that difference.
How to Prevent Acne Scars from Forming
The most effective approach is to prevent scars before they form.
Control active acne early. The South Indian hospital study found scarring in 56% of patients when acne lasted more than 3 years, versus 29.5% when it lasted less than 3 years. Duration directly correlates with scarring — early treatment matters.
Concrete behavioural steps:
- Never pick, pop, or squeeze pimples — this pushes bacteria deeper, worsens inflammation, and directly increases scarring risk
- Apply broad-spectrum sunscreen daily to active breakout areas to prevent PIH from darkening
- Treat nodular or cystic acne aggressively with medical care — don't wait it out
- Seek professional treatment at the first signs of moderate-to-severe acne, before deep tissue damage occurs
Treating established scars is far more complex and costly than preventing them. If scars have already formed, the sections below cover the clinical options available — from chemical peels and laser toning to RF microneedling — that a dermatologist can tailor to your skin type and scar pattern.
Frequently Asked Questions
What is the main reason for acne?
Acne is primarily caused by excess sebum production, clogged hair follicles, and the proliferation of Cutibacterium acnes bacteria. Hormonal changes (particularly androgens), stress, diet, and genetic susceptibility can all trigger or worsen breakouts.
Can acne scars be completely removed?
Most acne scars are permanent structural changes to the skin, and complete removal isn't guaranteed. Clinical treatments can significantly reduce depth and visibility — RF microneedling reduced mean scar scores by 34.35% in one Indian study, while microneedling studies report 51–60% improvement.
What is the difference between acne marks and acne scars?
Acne marks (PIH) are flat discolorations that fade on their own over weeks to months without structural treatment. True acne scars involve physical changes to skin texture — pitting or raised tissue — that require active clinical intervention to improve.
Which acne scar treatment is best for darker Indian skin tones?
Non-ablative lasers, RF microneedling, conservative chemical peels, and subcision are generally safer for Fitzpatrick IV–VI skin. Ablative lasers carry higher PIH risk and require careful patient selection. A dermatologist experienced with melanin-rich skin should always guide treatment selection.
How many sessions of microneedling are needed for acne scars?
Most protocols involve 4–6 sessions spaced several weeks apart, with improvement building over months as collagen remodelling progresses. RF microneedling platforms like Morpheus8 Pro may deliver meaningful results in fewer sessions due to deeper tissue stimulation.
How long does it take to see results from acne scar treatment?
Superficial peels may show improvement within a few weeks, while microneedling and RF microneedling results build over 3–6 months as collagen remodelling occurs. A complete treatment course — not just a single session — is what produces lasting results.