Key Takeaways
- Chemical peels treat melasma by exfoliating pigmented skin layers and disrupting melanin accumulation
- Peel choice depends on your melasma depth, skin tone, and Fitzpatrick type
- Indian skin (Fitzpatrick IV–VI) needs gentler, superficial peels with proper priming to avoid post-inflammatory hyperpigmentation
- Expect 4–6 sessions spaced 2–4 weeks apart before seeing meaningful improvement
- Daily broad-spectrum SPF is non-negotiable — a 2015 randomised trial found relapse rates of 54% without visible-light protection versus 18% with it
What Is Melasma and Why Is It So Hard to Treat?
Melasma is an acquired pigmentation disorder causing symmetrical brown or grey-brown patches on sun-exposed areas — cheeks, forehead, upper lip, and nose. It results from overactive melanocytes producing excess melanin, often triggered by UV exposure, hormonal shifts (pregnancy, oral contraceptives), thyroid dysfunction, stress, or genetics.
India's intense year-round sun makes this condition especially prevalent. Indian clinic data consistently shows that roughly 76–80% of melasma patients are women, most between 21–40 years old.
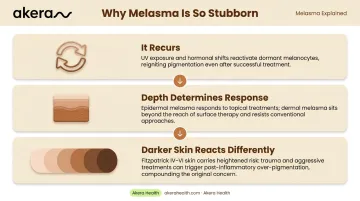
Three factors make melasma notoriously stubborn:
- It recurs: UV exposure or hormonal shifts can reactivate melanocytes even after successful treatment
- Depth determines response: Epidermal melasma responds well to peels, but dermal and mixed-type melasma sit deeper and resist surface-level treatment
- Darker skin reacts differently: Fitzpatrick IV–VI skin (the most common phototype in India) can overproduce pigment in response to trauma, so aggressive treatment risks making pigmentation worse
This is why the choice of peel, concentration, and provider matters as much as the treatment itself.
How Chemical Peels Work for Melasma
Chemical peels work by exfoliating the outer skin layers — shedding melanin-rich cells and prompting the skin to regenerate with more even pigmentation underneath.
The Mechanism Behind Pigment Reduction
Peels work on melasma through two main pathways:
- Physical removal of melanin-rich keratinocytes in the epidermis
- Disruption of melanin transfer — peels interrupt the cycle of melanin accumulation by clearing surface cells before new pigment can deposit
Medium-depth peels go further, reaching the papillary dermis and stimulating collagen alongside pigment reduction. For Indian skin (Fitzpatrick types IV–VI), though, this deeper injury significantly raises the risk of post-inflammatory hyperpigmentation — which is why most dermatologists keep melasma treatment at the superficial level.
Which Type of Melasma Responds Best
| Melasma Type | Response to Peels |
|---|---|
| Epidermal | Best response — peels directly target superficial melanin |
| Mixed | Partial improvement — the epidermal component responds, dermal is resistant |
| Dermal | Poor response — peels cannot reliably reach deeper pigment without unsafe trauma |
Priming: The Step Most Patients Skip
Using a priming agent for 2–4 weeks before your first peel significantly improves outcomes and reduces PIH risk. A 2008 Indian randomised trial of 60 melasma patients found that hydroquinone priming produced measurably better MASI score reductions than either tretinoin priming or no priming at all — at both six and nine months post-treatment.
Common priming agents include hydroquinone, retinoids, and kojic acid. Which one suits you depends on your skin's sensitivity — something your dermatologist will assess before your first session.
Types of Chemical Peels Used for Melasma
Peel selection depends on your melasma depth, skin tone, sensitivity, and Fitzpatrick type. A dermatologist assessment before your first session is essential.
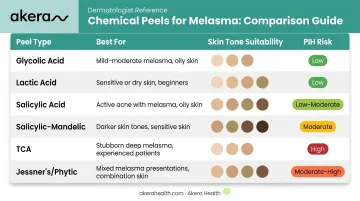
Here's a quick reference before diving into each option:
| Peel Type | Best For | Skin Tone Suitability | PIH Risk |
|---|---|---|---|
| Glycolic Acid | Epidermal & mixed melasma | Fitzpatrick I–IV | Moderate |
| Lactic Acid | Sensitive / reactive skin | All types | Low |
| Salicylic Acid | Oily / acne-prone + melasma | Fitzpatrick III–VI | Low |
| Salicylic-Mandelic | Ethnic skin, mixed melasma | Fitzpatrick IV–VI | Low–Moderate |
| TCA | Stubborn / deeper melasma | Fitzpatrick I–III | High |
| Jessner's / Phytic | Reactive or treatment-resistant | Varies | Low–Moderate |
Glycolic Acid Peel (AHA)
The most extensively studied peel for melasma. Used at concentrations of 30–70%, it exfoliates the uppermost skin layers, reduces surface melanin, and improves overall tone. A 2016 Indian RCT involving 90 patients found 62.36% MASI reduction with 35% glycolic acid after four weeks of priming and sessions every 14 days.
Best for epidermal and mixed melasma. Safe for darker skin at lower concentrations with proper neutralisation.
Lactic Acid Peel (AHA)
A milder AHA derived from milk, lactic acid is well-tolerated by sensitive and darker skin types. It penetrates more slowly than glycolic acid, which reduces irritation risk — and its mild moisturising properties make it useful when the skin barrier is already compromised. For patients new to peels or dealing with reactive skin, this is often the most appropriate starting point.
Salicylic Acid Peel (BHA)
Salicylic acid's anti-inflammatory properties set it apart from standard exfoliating peels. While most acids work through surface exfoliation alone, salicylic acid also dampens the skin's trauma response, which directly reduces post-inflammatory hyperpigmentation (PIH) risk. This makes it particularly well-suited to darker skin tones and cases where melasma coexists with oily or acne-prone skin.
Salicylic-Mandelic Combination Peel
Mandelic acid has a larger molecular size, meaning it penetrates more slowly and evenly — a property that makes it ideal for ethnic and sensitive skin. Combined with salicylic acid, the pairing delivers meaningful pigmentation improvement with a gentler side-effect profile than glycolic alone. The same 90-patient Indian RCT showed a 60.98% MASI reduction — comparable to glycolic acid but generally better tolerated in Indian skin.
This combination is increasingly preferred in clinical settings serving South Asian patients.
TCA (Trichloroacetic Acid) Peel
A medium-depth peel effective for stubborn pigmentation due to deeper penetration. Used at low concentrations (10–35%), it can reach mixed and deeper epidermal disease. The trade-off is significant — PIH and scarring risk is considerably higher in Fitzpatrick IV–VI skin. For Indian skin tones, most dermatologists reserve TCA for cases where gentler formulations have underperformed, and only under careful clinical supervision.
Combination and Newer Peels
For challenging or reactive cases, multi-acid formulations provide more flexibility:
- Jessner's solution (resorcinol + salicylic + lactic acid) combines keratolytic and anti-inflammatory effects
- Phytic acid peels require no neutralisation, reducing the risk of over-peeling
- Customised multi-acid blends allow dermatologists to calibrate depth and tolerance for individual skin profiles
These options are increasingly used when standard peels have underperformed or when sensitivity limits single-acid approaches.
What to Expect During and After a Chemical Peel Session
The In-Clinic Process
A standard session follows this sequence:
- Skin cleansing and degreasing to remove oils and ensure even penetration
- Peel application (mild tingling or stinging is normal; intensity depends on acid type and concentration)
- Dwell time monitoring as the peel sits for a set period under the dermatologist's supervision
- Neutralisation (required for glycolic acid) or self-neutralisation depending on the formulation
- Calming application with a moisturiser and broad-spectrum sunscreen applied before you leave

Sessions typically take 30–60 minutes. Akera Health's chemical peel services start from ₹3,000, with the exact cost depending on the peel type selected during your personalised consultation.
The Recovery Phase
What to expect in the days following a superficial peel:
- Days 1–2: Mild redness and tightness
- Days 3–5: Dryness, flaking, or peeling as the skin exfoliates
- Days 5–7: Skin settles and the refreshed surface becomes visible
Do not pick at peeling skin. Disrupting the natural shed increases PIH risk significantly in darker skin types.
Post-Peel Non-Negotiables
Protecting your skin after a peel is as important as the peel itself. Avoid until fully healed:
- Makeup, harsh exfoliants, and scrubs
- Retinoids and vitamin C serums (they can irritate compromised skin)
- Direct sun exposure without protection
Use daily:
- A gentle, fragrance-free cleanser
- A fragrance-free moisturiser
- High-SPF broad-spectrum sunscreen. Akera Health's Bask Sunscreen SPF 50+ comes in variants for oily/combination, normal, and dry/sensitive skin so you can match it to your skin type
Results and Long-Term Maintenance
Setting Realistic Expectations
Chemical peels produce gradual improvement, not instant transformation. Based on clinical trial data:
- After 1–2 sessions: Initial brightening and mild tone improvement
- After 3–4 sessions: Measurable reduction in melasma patch visibility
- After a full course (4–6 sessions): Most significant results for epidermal and mixed melasma
A 2020 Indian split-face study following 30 women after four glycolic peel sessions found 26.6% had clinical recurrence within three months, despite routine sunscreen advice. This reinforces that peels manage melasma, they do not cure it.
Why Maintenance Matters
Peels remove existing melanin but do not permanently switch off melanocyte activity. Without ongoing management, melasma returns, particularly with sun exposure or hormonal fluctuations.
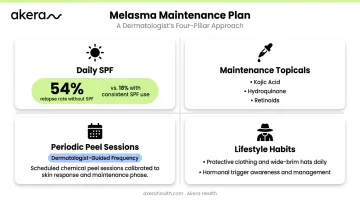
A maintenance plan typically includes:
- Daily SPF: Use a broad-spectrum sunscreen that covers visible light wavelengths, not just UV. Sunscreens protecting against visible light show a 54% six-month relapse rate versus 18% for UV-only formulas — a clinically meaningful difference for melasma patients
- Maintenance topicals: Kojic acid, prescribed hydroquinone, or low-dose retinoids between peel courses
- Periodic peel sessions: Your dermatologist determines frequency based on how your skin responds over time
- Lifestyle habits: Sun-protective hats and clothing; discuss hormonal contraceptive use with your doctor if it's a known trigger
At Akera Health, Dr. Lavina Mittal (MBBS, MD) evaluates each patient's melasma type, skin tone, hormonal background, and lifestyle before recommending a peel formulation, concentration, and session schedule. A consultation is the starting point for any melasma patient, because the right protocol depends entirely on your skin profile.
Frequently Asked Questions
Can a chemical peel get rid of melasma?
Chemical peels can significantly reduce the appearance of melasma (particularly the epidermal type) but do not permanently eliminate it. Melasma is a chronic condition prone to recurrence, so ongoing sun protection and maintenance treatment are required to sustain results.
How many chemical peels do I need for melasma?
Most patients require 4–6 sessions spaced 2–4 weeks apart for visible improvement. The exact number depends on your melasma's depth, your Fitzpatrick skin type, and how well your skin responds to the initial sessions.
Can melasma be permanently removed?
Melasma cannot be permanently eliminated: genetics, UV exposure, and hormonal activity all drive it and persist throughout life. It can, however, be effectively managed with consistent treatment, daily SPF use, and avoidance of known triggers.
Are chemical peels safe for darker Indian skin tones?
Yes, when performed by an experienced dermatologist. Glycolic acid, lactic acid, salicylic acid, and salicylic-mandelic peels have documented safety data for darker skin tones. Medium-to-deep peels carry a higher PIH and scarring risk for Fitzpatrick IV–VI skin and require careful clinical assessment.
What is the downtime after a chemical peel for melasma?
Superficial peels typically involve 3–5 days of mild redness and peeling. Medium-depth peels may require 5–7 days of recovery. Most patients resume normal activities within a few days, provided they follow post-care instructions and apply sunscreen diligently.
How long does it take to see results from chemical peels for melasma?
Initial brightening may be visible after the first 1–2 sessions. Noticeable improvement in melasma patches appears after 3–4 sessions, with full results assessed at the end of the complete treatment course.