That uncertainty is one of the most common skin dilemmas people face. Most moles are completely harmless, but some changes genuinely warrant professional attention — and knowing the difference matters.
This guide covers how to recognise a concerning mole using the ABCDE self-check method, the professional removal options available (and what each one actually involves), and why the choice of provider affects far more than just the cosmetic result.
Key Takeaways
- Any change in a mole's size, shape, colour, or texture warrants a dermatologist's evaluation before removal
- Choose from shave excision, surgical excision, cryotherapy, or RF cautery — the right method depends on the mole's depth, size, and location
- DIY removal (creams, acids, sharp tools) risks infection, scarring, and a missed cancer diagnosis
- Histological testing of removed tissue is only possible when a qualified dermatologist performs the procedure — not with DIY methods
What Are Moles and Why Do They Form?
Moles — medically called naevi, sometimes referred to as beauty spots — form when melanocytes (the skin's pigment-producing cells) cluster together rather than spreading evenly across the skin. They can be flat or raised, range from pale pink to deep brown or black, and appear anywhere on the body.
According to the National Cancer Institute, most adults have between 10 and 40 common moles. The majority are completely benign and never need medical attention. Some moles are present from birth; most develop during childhood and early adulthood, with new moles possible up to around age 40.
Common Moles vs. Atypical Moles
These two categories behave quite differently:
- Common moles are small, round, evenly coloured, and pose minimal risk
- Atypical moles (dysplastic naevi) are larger, irregularly shaped, and sometimes have uneven colour — roughly 1 in 10 people has at least one
- Having more than five dysplastic naevi is associated with approximately 10 times the melanoma risk compared to having none
Even so, individual moles — atypical or otherwise — only rarely become melanoma. The real concern is cumulative risk across multiple moles, not any single one in isolation.
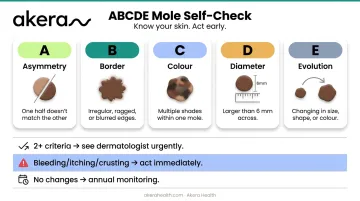
How to Tell If a Mole Needs Medical Attention: The ABCDE Rule
Dermatologists worldwide use the ABCDE framework as a practical triage tool — something anyone can apply at home to decide whether a mole warrants professional review.
Asymmetry and Border
A — Asymmetry: A benign mole looks roughly the same on both halves. If one half doesn't mirror the other, that's worth having checked.
B — Border: Healthy moles have smooth, well-defined edges. Ragged, irregular, or blurred borders can signal a problem.
Colour and Diameter
C — Colour: A normal mole is a single, uniform shade. Multiple colours within one mole — tan, brown, black, red, or white patches — warrant attention.
D — Diameter: Moles larger than 6mm (roughly the width of a standard pencil) are more likely to be atypical. Importantly, the American Academy of Dermatology explicitly notes that melanomas can be smaller than 6mm — so diameter alone isn't a safety threshold.
Evolution
E — Evolution is often the most important signal. Any mole that changes in size, shape, colour, or texture — or begins to bleed, itch, or crust — should be evaluated promptly, even if it looks otherwise unremarkable.
When to act vs. when to monitor:
- Two or more ABCDE criteria → see a dermatologist urgently
- Any bleeding, itching, or crusting → don't wait
- No changes, no symptoms → annual monitoring is generally sufficient
Self-checks are a starting point, not a diagnosis. A dermatologist uses a dermatoscope — a specialised magnification tool — to assess moles with far greater accuracy than the naked eye. A 2018 Cochrane review found that dermoscopy combined with visual inspection achieved 92% sensitivity versus 76% for visual inspection alone. In practice, that 16-point difference can mean catching a melanoma that a naked-eye check would miss.
Mole Removal Options: What Dermatologists Actually Use
A dermatologist assesses the mole's size, depth, location, and any cancerous risk before recommending a technique. The method matters beyond cosmetics: tissue removed should be sent for histological analysis, which is only possible when the specimen is preserved intact.
Shave Excision
After local anaesthesia, a surgical blade shaves the raised portion of the mole flush with the surrounding skin. No stitches are needed. RF cautery (radiofrequency energy) may be used alongside to control bleeding and reduce regrowth risk.
- Best for: small, raised, benign moles
- Scarring: usually minimal
- Limitation: may leave deeper naevus cells; a 2022 prospective study reported recurrence in 33% of treated naevi at 6–12 week reviews
Surgical Excision
The entire mole and a small margin of surrounding skin are removed with a scalpel and the wound is sutured closed. This is the standard approach for suspicious, deep, or larger moles — because it preserves an intact tissue specimen for biopsy.
- Best for: deeper moles, larger moles, or any with suspected malignancy
- Scarring: a linear scar is likely but typically fades with proper aftercare
- Key advantage: full histological assessment is possible
Cryotherapy
Liquid nitrogen freezes and destroys superficial mole tissue. Quick to perform, but it destroys the tissue — meaning no specimen for histology.
- Best for: small, shallow, non-cancerous spots only
- Not appropriate if cancer is any concern
RF Cautery (Electrocautery)
High-frequency radiofrequency energy targets and removes benign skin growths with minimal damage to surrounding tissue. At Akera Health in Bengaluru, RF cautery is used as part of the mole removal toolkit — particularly for raised, benign lesions — alongside shave excision and surgical excision. The method selected depends on the mole's characteristics and any clinical concerns identified at consultation.
One clinical rule applies across all methods: destructive techniques (cryotherapy, cautery) are appropriate only for confirmed benign lesions. Suspicious or changing moles require a method that preserves tissue for biopsy.

Laser treatment is a notable example of where this matters — a retrospective series of 12 patients found that prior laser treatment complicated or delayed melanoma diagnosis in all cases reviewed, because no intact specimen remained.
Why You Should Never Remove a Mole Without a Dermatologist
The risks of DIY removal go well beyond a bad cosmetic result.
Physical dangers of at-home removal:
- Using scissors or blades risks serious infection and permanent scarring
- Incomplete removal often causes regrowth
- Home remedies — apple cider vinegar, mole removal creams, essential oils — have no clinical evidence behind them
One published case documented a 14-year-old who developed erosions and a chemical burn after applying apple cider vinegar under occlusion to two naevi for just three days. A 2023 study identified 38 injury cases linked to unapproved topical removal products, including burns, scarring, ulceration, and infection — with the same study confirming there are no FDA-approved drugs indicated for mole removal.
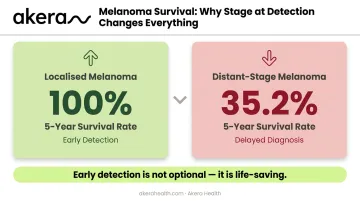
The diagnostic risk matters just as much. You cannot tell whether a mole is cancerous by looking at it. Removing it at home destroys the tissue needed for biopsy, delaying a diagnosis that could be life-saving. SEER data show 100% five-year survival for localised melanoma versus 35.2% for distant-stage melanoma — numbers that show exactly what early detection is worth.
Beauty salons and non-medical clinics carry the same risk. Laser or dermabrasion treatments performed by untrained practitioners bypass proper diagnosis and post-removal tissue analysis. Even if the cosmetic result looks fine, there is no clinical accountability and no histological safety check. Only a dermatologist-performed removal ensures the right technique — and the medical oversight to act on what the biopsy shows.
What to Expect Before, During, and After Mole Removal
Before the Procedure
A dermatologist will examine the mole visually and discuss your health history, including any changes you've noticed and relevant family history of skin cancer. Your dermatologist will explain the recommended removal method and expected outcome before anything proceeds. If there's any clinical concern, a biopsy may be recommended before full removal.
During the Procedure
Most in-clinic mole removals are performed under local anaesthesia. Depending on the method and the mole's complexity, procedures can take anywhere from 15 minutes to one hour, with most patients needing to allow around 1.5 hours for the full visit. You'll feel numbness and possibly mild pressure — light bleeding and redness immediately afterwards are normal.
After the Procedure
Once the procedure is complete, following your dermatologist's aftercare instructions closely helps ensure smooth healing and minimal scarring. Standard aftercare typically includes:
- Keeping the site clean and dry
- Applying prescribed ointment and a fresh dressing daily
- Avoiding direct sun exposure — particularly important in Bengaluru, where the UV index regularly reaches the 'very high' to 'extreme' range year-round, making post-procedure skin more vulnerable to pigmentation changes
- Monitoring for infection signs: worsening pain, increasing swelling, warmth, pus, or fever
- Stitch removal (if applicable) within one to two weeks
Mild redness or pigmentation changes at the site are normal and typically fade within 4–12 weeks. Sun protection with a broad-spectrum SPF 50+ sunscreen — applied consistently once the wound has healed enough — is one of the most effective ways to minimise long-term scar visibility.
Frequently Asked Questions
How can I remove beauty spots?
Beauty spots should only be removed by a qualified dermatologist using methods such as shave excision, surgical excision, or cryotherapy. A proper diagnosis must come first to rule out malignancy — the removal method follows from that assessment, not the other way around.
Can I remove moles without surgery?
Yes — non-surgical options like cryotherapy and RF cautery exist for small, benign, superficial moles. A dermatologist must first confirm the mole is non-cancerous. "Non-surgical" does not mean "at home" — these are still clinical procedures requiring professional equipment and oversight.
Does mole removal leave a scar?
Some degree of scarring is possible with most methods, though shave excision and RF cautery tend to leave minimal marks. Scars tend to fade over time, particularly with consistent sun protection and proper wound care.
How many sessions does mole removal take?
Most benign moles are removed in a single procedure. When multiple sessions are needed, it depends on the mole's depth, pigment, and the method used. Your dermatologist can give a realistic estimate at your consultation.
When should I see a dermatologist about a mole?
Any mole matching one or more ABCDE criteria — or that bleeds, itches, or changes noticeably — should be evaluated promptly. Even without warning signs, an annual skin check is recommended, particularly for anyone with many moles or a family history of melanoma.